Many thanks to Dr Tom Kirk for this response to the Prime Minister's letter to doctors in England.
Firstly, the patronising "myth-busting" tone used in this letter is disgraceful when addressing professionals. Instead of acknowledging the issues and problems with his rushed plan on a level basis, he seeks to instruct us where we are wrong. As other commentators have pointed out, how his training in PPE prepares him for the largest reorganisation of the world’s third biggest employer is lost on me – but apparently Dave knows it all.
The myths as he puts them are only there because the white paper is as vague as possible - to allow for post implementation changes to suit and woo private investment - such as large scale privatisation and hospital closure.
Response to "Dave's Myths"
Myth 1 – NHS is fine as it is
Dave says change is necessary.
This is a statement of fact, but not an indication of the needed direction of change. To state that change is necessary in health care is stating the blindingly obvious - its probably one of the fastest changing industries there is. However, this is not an excuse to rush through untried ideologically-based ideas.
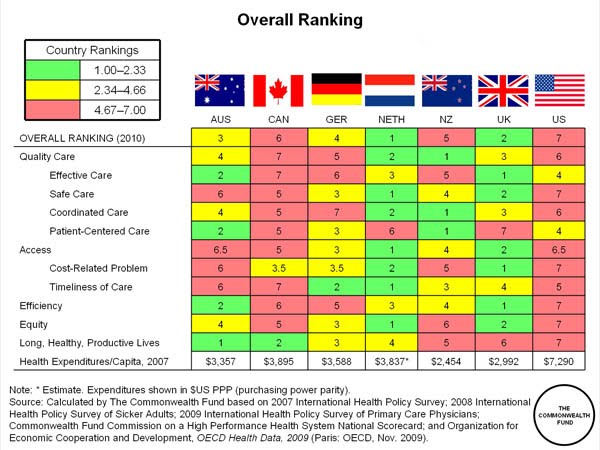
The phrase "despite spending the European average on health, some of the outcomes are poor in comparison" is particularly odious. Yes, levels reached in spending do hit the enlarged EU average, and yes we are not top of the league table for all outcome data (though we are top, or near top for a fair few).
But here is a list of countries which spend more than the UK (8.7) as a percentage of GDP on health.(1)
France 11.2
Switzerland, Austria, Germany -c 10.2
Belgium, Portugal, Denmark, Greece -c 9.7
Iceland, Netherlands, Spain, Sweden - c 9.1
What's more levels of spending in these countries have been at these levels for a while, and most of the data the Dave is quoting uses 5 year survival data. With time for follow up, gathering a cohort, and analysis the lag is probably in the region of 10 years.
So, here is what Dave is doing. He is judging the NHS on results 5-10 years old, obtained when levels of spending in the comparator countries was substantially greater than NHS spending.
Even if "Dave’s" analysis wasn't completely flawed, and we aren't ahead in all areas relative to spending - demographical differences (obesity, diet etc) account for most of the apparent health inequalities.
If we go along with Dave for a second time, and say that we do have the same historical spending as the EU average, and the same demographic make up, he offers us no compelling reason to accept his model for future care over any other one.
Repeated non partial analysis of health care systems have found that the most efficient care systems are ones that don’t involve private companies, have a single payer (government), don’t waste money on duplication, and don’t waste time on calculating the exact cost of every ‘health interaction’. (2,3, 4)
Of interest is the prediction (2) in 2008 that a government will come in, use the word “unsustainable” to describe current funding arrangements, and then force through unwanted change on the back of this.
Indeed a recent health committee report entitled “20 years of costly failure” recently asked the question: What benefit has commissioning brought? It is hard to establish what the benefits are, if they exist, and if they outweigh the significant outlay in cost and time that has been put into the commissioning process.
It is all ideologically driven changes - as the son of Thatcher he thinks that anything private is better than anything public.
Myth 2 – Plans out of blue
Dave says: Plans not out of the blue.
All Dave offers here is “I disagree”, followed by comparisons to failed fundholding, and commissioning under the labour government, glossing over the largest ever change to the structure of the NHS, and abolition of most of the management structure.
“Our plans simple build on these advances” – yes in the same that Marxism simple builds on the idea that sharing is good.

How much of this not-out-of-the-blue change was in your plan, Dave?
– That the plans are untested and implemented too fast
Dave says
things aren’t untested and too fast.
Dave’s argument here is that its two years in the future – on the assumption that two is clearly enough time to do anything. He glosses over the fact that there are no significant trials of this system that show it works, and that it’s all based on guess work.
In the process he is making a mockery of the carefully built evidence base that has been assembled, and is completely giving up on the noble ideas of evidence-based policy – returning the NHS to a political football.
Myth 4 – GPs will spend all their time on paperwork.
Dave says
not true.
GPs will apparently be given extra resources to cover this part of the job. Presumably these extra resources will come from those saved by axing all the PCTs. Oh hang on – wasn’t there an analysis that stated that it will actually cost money to axe the PCTs? The response Walsh published suggested that the cost of reorganisation will cost 2-3 billion, and that even if the savings come in as planned, which is unlikely, we will still be spending more money than saving this parliament.(5) So the money for the extra staff needed for this will come from the clinical budget then.
Myth 5 – That GP’s will be forced to work with Private health sector companies to help them with commissioning.
Dave says
nothing could be further from the truth.I believe him on this. GPs won’t be forced to work with private companies. They won’t have to be forced. With PCTs and SHAs gone, there won’t be anyone else but private companies. No forcing from government is required as the practicalities and the situation they have created will do it for them.
One more thing mentioned in the letter by David Cameron is the repeated use of phrases such as giving the professional “much more freedom to care for patients in the way you decide is best”.
It is clear that this freedom will relate to a small group of influential GPs in each of the consortia who will set local agendas. Already my local consortium is sending various money-saving "tips" to each practice, and the constructing tables and graphs of each practice performance of these.
An example is statin prescribing and the percentage use of simvastatin over all others. The ranking, use of encouraging language and style all give the impression that those practices prescribing the highest percentage of statins as simvastatin are the ones that are succeeding and doing the right thing. This is not true from a patient point of view, with those practices excelling at cholesterol management and prevention of heart attacks likely to appear at the bottom of the list. This extreme budgetary focus will negatively impact patient care, and encourage price control over patient benefit.
I fear that where PCTs were unwilling to interfere with clinical decisions, the leaders of the consortia will not have the same reluctance. Whether this is a good thing or not is debatable. Whether this leads to setting the professional free is not a debate - it will only restrict the abilities of day-to-day GPs and hospital doctors.
Of interest are a number of things NOT mentioned in the letter:
1) What happens when GP consortia fail? This is bound to happen as whichever formulas they use to work out budgets, some area will have a natural deficit. On top of this some areas will inherit deficits that may make budgets unworkable.
a. Answer is – they will be taken over as failing consortia by private health companies
2) What happens to training, when all easy and profitable routine work is contracted out to private companies?
a. Training will worsen, doctors will become under-skilled, patients will lose out.
3) What happens to NHS hospitals and departments if they are outbid by private providers?
a. Answer is – they will close, and give a nearly complete local monopoly to the private provider
References
1)
http://www.ingentaconnect.com/content/oecd/16080289/2010/00002010/00000021/8110161ec043;jsessionid=1i6jeq11hmqhu.alexandra
2)
http://www.bmj.com/content/336/7658/1410.full?rss=13)
http://www.parliament.uk/business/news/2010/03/20-years-of-costly-failure-mps-verdict-on-nhs-commissioning/4)
http://www.bmj.com/content/342/bmj.d7.full?sid=a3f1af1d-d547-46cb-8495-f908459e15105)
http://www.bmj.com/content/341/bmj.c3843.full

 By next year our heart attack deaths will be lower than those in France. OK. Dr Grumble knows. There is more to this than health care. But this example should never have been used to slag off our NHS. Two can play at this game, Dave.
By next year our heart attack deaths will be lower than those in France. OK. Dr Grumble knows. There is more to this than health care. But this example should never have been used to slag off our NHS. Two can play at this game, Dave.



{kind=link}
{kind=link}